The Shoulder
Anatomy of the Shoulder
The shoulder joint, or more properly the glenohumeral joint, is the articulation or joint between the head of the humerus (the arm bone) and the glenoid (part of the scapula or shoulder blade. The humeral head is the ‘ball part of the joint and the glenoid is the ‘socket’ part of the joint. The clavicle or collar bone acts as strut between the sternum (breastbone) and the scapula and attaches to the scapula at the acromioclavicular joint.
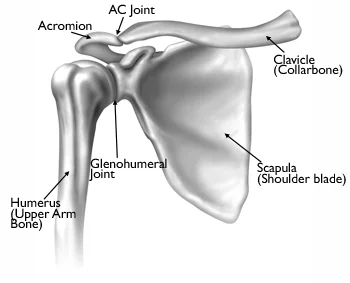
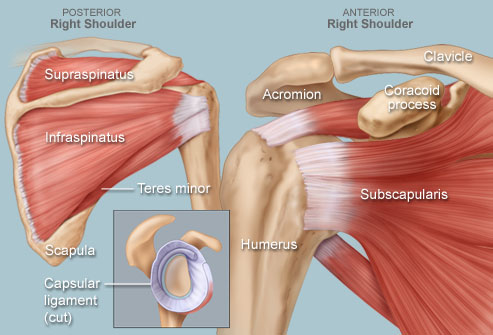
The humeral head is nearly half a sphere. It points slightly upwards and backwards towards the glenoid. The glenoid is small and shallow about a 1/3 of the surface area of the humeral head. This anatomical arrangement allows the shoulder to be the most mobile joint in the body, which is good for placing the hand where you want it to be, but at the cost of being the most unstable large joint in the body. There are both static and dynamic factors that help control shoulder stability. The static structures providing stability to the joint are the labrum (a rim of gristle or cartilage attached to the rim of the glenoid), the joint capsule and ligaments. The dynamic factors providing shoulder stability are the muscles around the shoulder in particular the four rotator cuff muscles. They are the supraspinatus, infraspinatus, teres minor and subscapularis. Their job is to stabilize the humeral head in the socket and to assist in elevation and rotation of the shoulder. The portion of a muscle that attaches to bone is referred to as a tendon, and the rotator cuff has four tendons, which are located in a small space between the humeral head and the acromion.
These muscles also provide strength to the shoulder together with the deltoid muscle on the outside of the shoulder and the muscles around attaching the shoulder blade to the chest wall and spine. The deltoid muscle is a large powerful muscle, which attaches the shoulder blade and collarbone to the arm bone. Its function is to lift, flex and extend the shoulder joint. It provides most of the power in the shoulder.
Other muscles that attach near the shoulder include the latissimus dorsi in the back and the pectoralis major in the chest. These large muscles act to internally rotate the humerus.
The acromioclavicular joint is made up of the collarbone and a part of the shoulder blade called the acromion. It is located almost directly over the glenohumeral joint. In contrast to the glenohumeral joint, there is very little motion at this joint. It is held together by the acromioclavicular and coracoclavicular ligaments. Injuries to these ligaments are known as a 'separated shoulder'.

The sternoclavicular joint connects the collarbone to the sternum, or breastbone, and helps support the shoulder. It is rarely injured, except in high-velocity trauma, but arthritis may develop in the joint leading to the appearance of a tender bump where the bones connect.
Any of these structures can be damaged either through injury, overuse or wear and tear. Shoulder pain is common and is the third most common cause of musculoskeletal consultation in primary care.1% of adults consult their GP each year with new shoulder pain and the self-reported prevalence of shoulder pain is between 16% and 26% (i.e 16%-26% of adults have shoulder pain at any one time).
What causes shoulder pain?
The shoulder is the most mobile joint in the body. The main shoulder joint is a ball-and- socket joint, which allows a very wide range of movement. A group of four muscles and their tendons make up the rotator cuff, which controls movement and also helps to hold the joint together.
There are many causes of shoulder pain, but the most common reason is related to the rotator cuff. These muscles have to work with every arm activity we do day to day. Sometimes, due to overuse, a change in activity or just normal age related changes these muscles don’t do their job as well which can result in pain.
The good news is that if you have shoulder pain that has come on gradually or without any history of trauma then simple exercises that help these muscles work better can help get your pain better.
What are the symptoms?
- Pain around the front and/or side of the shoulder.
- Spontaneous or gradual onset
- Pain is made worse by movement, e.g. raising arm above shoulder level or the action of putting on a coat. Some people will complain of pain at night, particularly when lying on the affected side.
Diagnosing Shoulder Pain
There are many causes of shoulder pain but generally, as long as you haven’t had a history of a fall or injury most shoulder pain responds well to exercises that make the rotator cuff muscles stronger. Half of all first time episodes of shoulder pain get better without treatment in 6 to 12 weeks.
X-rays and other investigations are not usually necessary during the first episode of pain. They are only indicated if you fail to respond to the advice and exercises recommended below: